Optimal testosterone after 40 is one of the most misunderstood topics in men’s health. People often assume fatigue, low drive, stubborn fat, irritability, and slower recovery are “just aging.” They are not. These are hormonal symptoms, not personal failings — and testosterone is often the missing piece.
Testosterone affects:
✅ Muscle mass and strength
✅ Metabolic flexibility and fat distribution
✅ Sleep quality
✅ Libido and erectile function
✅ Mood stability and motivation
✅ Cognitive sharpness
✅ Long-term vitality and resilience
Once testosterone declines, the entire hormone web shifts — cortisol rises, thyroid function changes, insulin sensitivity drops, and GH/IGF-1 output decreases. This creates the classic over-40 cascade: less energy, more fat, slower recovery, and weakened drive.
This guide explains exactly what labs to order, what “optimal” means (not just “normal”), how lifestyle influences T, how GLP-1 drugs like Retatrutide affect hormones, and when supplementation or TRT becomes clinically appropriate.
Symptoms of Low Testosterone After 40 (Often Misdiagnosed)
Primary symptoms
✅ Loss of muscle mass or strength despite consistent training – Recovery feels slower, pumps feel weaker
✅ Increased abdominal fat or visceral fat – Waist circumference increases even without major weight gain
✅ Low libido or weaker erectile function – Morning erections decline
✅ Fatigue, especially afternoon crashes – Mitochondrial output decreases when testosterone is low
Cognitive and emotional symptoms
✅ Irritability, emotional flatness, or low mood – Dopamine signaling becomes impaired
✅ “Foggy” thinking, slower recall – Testosterone influences verbal memory and processing speed
Behavioral symptoms
✅ Reduced motivation or drive – Men often describe it as, “I just don’t feel like myself anymore.

Optimal Testosterone Ranges (Not “Normal” Ranges)
Reference ranges reflect an unhealthy population. Optimal ranges reflect where men feel and function their best.
Optimal targets for men over 40
✅ Total Testosterone: 700–1100 ng/dL – Symptom-guided adjustments still required
✅ Free Testosterone: upper third of lab range – Most predictive of mood, libido, strength, and vitality
✅ Bioavailable Testosterone: 200–300+ ng/dL
✅ SHBG: 20–40 nmol/L
🔹 Lower SHBG → more free T
🔹 High SHBG often accompanies low thyroid
If your SHBG is high or your energy feels “off” even with decent testosterone numbers, it’s worth looking at thyroid optimization over 40 alongside testosterone.
A controlled study showed that free testosterone, not total testosterone, is the strongest predictor of physical function and vitality.
→ Free Testosterone and Functional Outcomes in Older Men
Additional Hormones That Influence Testosterone Function
These markers are equally important for men over 40 but are rarely tested:
✅ DHEA-S – Mid to upper end of range – Supports energy, mood, immune function, and androgen production
✅ Pregnenolone – Middle of reference range – Precursor hormone for cognition, stress resilience, and memory formation
✅ DHT (Dihydrotestosterone) – Mid-range, symptom-guided – Supports drive, erectile quality, neurological sharpness
🔹 Too low = low libido and low confidence; too high = acne or scalp sensitivity
✅ Estradiol (Sensitive Assay): 20–35 pg/mL – Symptom-guided – Essential for libido, joint comfort, sleep, and cardiovascular balance
✅ Prolactin – Low-normal range – High prolactin can blunt libido, erectile function, and energy even if testosterone is normal
Labs You Should Ask Your Doctor For
🔹 Total Testosterone
🔹 Free Testosterone (Equilibrium Dialysis)
🔹 SHBG
🔹 Bioavailable Testosterone
🔹 Albumin
🔹 DHEA-S
🔹 Pregnenolone
🔹 Estradiol – Sensitive (LC/MS)
🔹 DHT
🔹 Prolactin
🔹 LH
🔹 FSH
🔹 CBC
🔹 CMP
🔹 Lipid Panel
🔹 Fasting Insulin + A1c
🔹 TSH, Free T3, Free T4, Reverse T3
This is the complete testosterone optimization panel, not the partial version most clinics order.
Need Help Getting Your Labs Ordered, Interpreted, and Optimized?
Most men receive incomplete hormone testing or outdated analysis. If you want a clinician-style, step-by-step review of what you need, what it means, and how to optimize it, I walk you through the entire process in my Health Optimization Consultation.
How Testosterone Influences Mood, Motivation & Cognitive Function
Primary effects on the brain
✅ Increased dopamine activity → higher motivation – Helps restore “drive”
✅ Improved stress resilience – Lower perception of overwhelm
✅ Faster cognitive processing – Improved verbal and working memory
Emotional effects
✅ Greater confidence and assertiveness – Not aggression — stability
Common psychological symptoms of low T
✅ Loss of competitiveness
🔹 Feeling “flat” or indifferent
✅ Procrastination and reduced initiative
🔹 Dopamine circuits underperform
A clinical review found testosterone replacement improved decision-making speed, mood resilience, and cognitive function.
→ Testosterone and Cognitive Function
Retatrutide, GLP-1 Physiology & Testosterone After 40
GLP-1 agonists (semaglutide, tirzepatide) and triple agonists like Retatrutide dramatically influence metabolic health — which means they also influence testosterone.
Positive effects of GLP-1 medications
🔹 Significant visceral fat reduction – Less aromatization → higher free testosterone
🔹 Improved insulin sensitivity – Better androgen receptor function
🔹 Decreased inflammation – More responsive LH → testosterone production improves
Many men on GLP-1s notice improvements in fat loss but plateaus in strength or libido. This is often due to suboptimal testosterone, which I break down in my guide to optimal testosterone after 40. Retatrutide’s profound visceral fat reduction makes it one of the most powerful indirect testosterone optimizers.
Temporary challenges to watch
🔹 Rapid weight loss may reduce cholesterol – Cholesterol is a precursor for testosterone synthesis
🔹 Appetite suppression → micronutrient gaps – Zinc, magnesium, vitamin D intake can fall
A weight-loss study demonstrated that losing visceral fat significantly elevates testosterone in men.
→ Effect of Weight Loss on Testosterone in Men
Lifestyle Strategies to Support Testosterone After 40
GLP-1 agonists (semaglutide, tirzepatide) and triple agonists like Retatrutide dramatically influence metabolic health — which means they also influence testosterone.
Strength Training
Strength training increases testosterone responsiveness even if testosterone levels don’t change.
Primary methods:
🔹 Heavy compound lifting (squats, deadlifts, presses, rows) – Maximizes androgen receptor expression
🔹 8–12 rep hypertrophy work – Ideal range for hormonal stimulation
Sleep Optimization
Primary improvements:
🔹 7.5–9 hours of consistent sleep
🔹 Most testosterone is produced in deep sleep
🔹Even one week of sleep restriction can drop testosterone 10–15%
Nutrition for Hormone Support
Primary strategies:
🔹 Adequate dietary fats – Cholesterol → pregnenolone → testosterone
🔹 High-protein diet – Supports lean mass and metabolic rate
Secondary considerations:
🔹 Zinc, magnesium, vitamin D, boron
🔹 Carbs around training to blunt cortisol
Stress Management
🔹 Lower chronic cortisol – Cortisol suppresses testosterone at multiple levels
For a deeper breakdown of how stress hormones blunt testosterone and what to do about it, read my guide on cortisol suppression of testosterone.
Body Composition
Primary driver:
🔹 Reduce visceral fat – Less aromatase activity → higher free T

Optimal Testosterone After 40: TRT Delivery Methods & What to Expect
Testosterone replacement therapy (TRT) is not a one-size-fits-all strategy. Delivery method determines absorption, symptom stability, estrogen conversion, and lifestyle convenience.
Testosterone Cypionate (Injectable)
Most common and most stable option.
Advantages
🔹 Predictable absorption
🔹 Long clinical history of safety
🔹 Works well for strength athletes
🔹 Flexible dosing (1–3x weekly)
Disadvantages – may cause slight peaks/troughs depending on injection frequency
Testosterone Enanthate (Injectable)
Nearly identical to cypionate with a slightly shorter ester.
Advantages
🔹 Smooth release
🔹 Good for men who aromatize more easily
🔹 Widely available
Disadvantages – may require slightly more frequent injections than cypionate
Subcutaneous Injections (Cypionate or Enanthate)
Injected into belly fat instead of muscle.
Advantages
🔹 Lower pain
🔹 Very steady absorption
🔹 Lower risk of hematocrit spikes
Disadvantages – not ideal for men with very low body fat
Transdermal Testosterone Cream (Scrotal Application)
Absorbed extremely efficiently due to skin permeability.
Advantages
🔹 Strong DHT boost (can improve libido and mood)
🔹 Smooth daily levels
🔹 No needles
Disadvantages – must apply daily – risk of transfer to others
Transdermal Shoulder Cream/Gel
Lower DHT conversion but convenient.
Advantages
🔹 Easy use
🔹 Stable levels when applied consistently
Disadvantages – lower absorption than scrotal application – risk of transfer
Pellets (Testopel)
Inserted under the skin every 3–6 months.
Advantages
🔹 Low maintenance
🔹 Consistent dosing
Disadvantages – surgical insertion – hard to adjust dose – high estrogen spikes common

Before TRT vs. On TRT — Comparison Table
| Category | Before TRT | On Optimized TRT |
|---|---|---|
| Energy & Drive | Low motivation, afternoon crashes | Stable energy, stronger initiative |
| Body Composition | Increased visceral fat, muscle loss | Lower fat, increased muscle retention |
| Libido & Erectile Quality | Reduced libido, inconsistent performance | Improved desire and erectile function |
| Cognitive Function | Brain fog, slower recall | Sharper memory and focus |
| Mood Stability | Irritability, emotional flatness | Improved resilience and emotional balance |
How Optimal Testosterone After 40 Shapes Hormone Interactions
Testosterone interacts with every major hormone system. This model explains why optimizing T requires optimizing the entire endocrine environment.
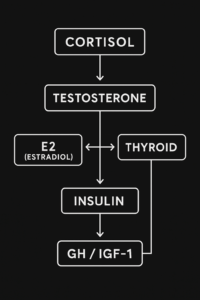
Interpretation:
🔹High cortisol suppresses testosterone signaling.
🔹Estradiol balance is essential for libido, joints, and mood.
🔹Thyroid function determines testosterone utilization.
🔹Insulin resistance reduces androgen receptor sensitivity.
🔹GH/IGF-1 decline worsens recovery and reduces testosterone’s anabolic effect.
Internal links will connect to your Thyroid Article, Cortisol Article, and upcoming Insulin Resistance and GH Decline articles.
Supplementation Framework for Testosterone Optimization
Supplements don’t replace TRT but support the entire hormonal ecosystem.
Foundational Supplements
✅ Vitamin D3/K2 – supports hormone production and LH signaling – Most men over 40 are deficient
✅ Zinc – essential for androgen production – Low zinc → decreased testosterone synthesis
✅ Magnesium glycinate or threonate – improves sleep and cortisol regulation – Better sleep → higher testosterone
Targeted Supplements
✅ Boron – may increase free testosterone by reducing SHBG – Typically 3–6 mg/day
✅ Omega-3 fatty acids – reduces inflammation – Higher systemic inflammation suppresses testosterone
Mitochondrial Support
Testosterone function depends heavily on cellular energy systems.
✅ Creatine – improves strength and anaerobic output – Better training → better hormonal response
✅ CoQ10 – supports mitochondrial electron transport – Energy production improves testosterone utilization
If you’re already dialed in on labs, training, and nutrition, advanced peptide protocols for men over 40 can further improve recovery, fat loss, and hormonal signaling.
Risks & Monitoring on TRT
Primary risks
🔹 Elevated hematocrit – requires monitoring every 3–6 months – Phlebotomy or dose adjustments may be needed
🔹 Elevated estradiol – symptom-based, not number-based – High = water retention, irritability
🔹Low = joint pain, low libido
Secondary physiological considerations
🔹 Lipid changes – lifestyle offsets most of this
🔹 Fertility suppression – HCG or enclomiphene may be needed
Ready to Rebuild Your Energy & Resilience?
Discover how hormone optimization, peptides, and functional lifestyle design can help you age actively—not passively. Your next chapter starts now.
Conclusion & Takeaway
Optimal testosterone after 40 is not about chasing a number — it’s about restoring the physiology that drives strength, motivation, metabolic flexibility, emotional resilience, and long-term vitality.
Men who optimize testosterone often describe the experience the same way:
“I feel like myself again.”
→ If you want the full systems map that shows how sleep, insulin, cortisol, inflammation, mitochondria, and hormones interact, start here: Hormones and metabolism after 40.
FAQs About Optimal Testosterone After 40
optimal testosterone after 40, testosterone levels after 40, TRT for men over 40, symptoms of low testosterone, testosterone lab testing, testosterone replacement therapy options